.jpg)



By Dezheen Zebari:
This paper (fully entitled ‘Infection Control and Prevention in the Health Care Setting in the Kurdistan Region of Iraq’) is based on research I conducted in Kurdistan in 2012. I’ve stayed in touch with multiple health care providers currently practicing in different cities who have told me things have not changed at all. My supervisor on the paper, Dr. Abdulrahman Tawfeeq Saadi*, has also stated that this article remains relevant.
Introduction:
Infection prevention and control procedures endeavor to ensure the protection of those who might be susceptible to acquiring an infection both in the general community and while receiving care due to health problems, in a range of settings. Infection control in developing countries can seem primitive depending on the region and the specific stage the health care facilities are functioning.
Health care associated or hospital-acquired infections (HAI) (nosocomial infections) are a worldwide problem. They represent infections acquired during or associated with delivery of care in contrast to infections present at the time of the care. Hospital-acquired infections are among the leading causes of death and they cause significant morbidity among patients who receive health care (EMS, 1). These complications of care often end up requiring expensive use of health care resources and lead to increased use of medication and supplies, to more laboratory studies, and to increased duration of hospitalization. They also may impair the quality of life of the patient with a Hospital acquired infections even after treatment. Prevention of Hospital- acquired infections is thus cost effective and achievable even when resources are limited.
Technologic advances and increased use of invasive procedures, patient populations that are getting older or are suffering more chronic diseases, and increasing proportions of patients with immune-compromised conditions or diseases are all factors that contribute to a greater identification and incidence of Hospital-acquired infections. Further, the prevalent use of antimicrobials, especially over- or inappropriate use of antibiotics, has contributed to an increased frequency of antimicrobial-resistant organisms which are often the culprits of Hospital-acquired infections. Factors linked with transmission of resistant strains of these microorganisms include lack of attention to hygiene, overcrowding, poor effective infection control program, and shortage of trained infection control providers .There is a misunderstanding that infection control programs are expensive and are therefore beyond the reach of most hospitals. In fact, the opposite is true. Infection control is based on common sense and on safe practice and can be implemented with minimal cost.
An effective infection control program will save the hospital an extensive amount of money. For example, high rates of sepsis among patients admitted to intensive care units can be controlled by thorough hand hygiene and by use of aseptic techniques rather than by prescribing expensive antimicrobials, which may further compound to the problem. Additionally, negligence to safe injection practices can result in iatrogenic transmission of blood-borne pathogens. Because a high proportion of those with HCV develop chronic infection, both morbidity and mortality from hepatitis C can be extended. High prevalence of this disease offers opportunity for continued HCV transmission, including risk to health care workers who may obtain injuries from contaminated sharps used for care of patients with chronic HCV infection.
The principles of infection prevention and control are the same throughout the world. Unfortunately, the discipline of infection control is poorly developed in areas such as Kurdistan where there is a rapidly developing health care system and where there is little expertise in infection control training. Establishing a cost effective program should become a leading priority for the Ministry of Health and is an essential component of efforts to improve the quality of health care.
The Kurdistan region has seen enormous growth in all sectors in a very short period of time. The health care setting should have seen the same development but such improvements have not been achieved in this field. By focusing a closer lens on infections that patients are predisposed to or may acquire as in-patients; it will allow one to determine where the problems are occurring. After such an endeavor, solutions to such issues can be evaluated and implemented to initiate a prevention campaign.
Methodology:
Data will be gathered in two districts of Kurdistan in major hospitals. These cities include Dohuk and Akre. By observing these regions, a comparative analysis can be accomplished. This will allow the interpreter the ability to establish the obstacles, available resources and needs of each region. The specific departments to evaluate are operating room and central sterilization department at Azadi Hospital in Dohuk, emergency department and operating room at Gulan Hospital in Akre.
Results:
To begin with, in Dohuk at Azadi hospital, the staff was dressed properly, no outside shoes or clothes were allowed into the Operating Unit, the patient was sterilized using iodine, and the surgical site was kept sterile most of the time. The OR temperature in each room was kept between 20 to 25 degree Celsius and humidity was kept around 30-40%. The room air is changed every couple of hours and the whole OR unit air is changed every Thursday. However, the staff wore open toed sandals in the OR which poses a great risk for injury and exposure to infections. Some of the surrounding staff and those directly operating on the patient would have their face mask off and handled hazardous waste without gloves. Most of the staff in the OR unit are not properly immunized and those that are have no proof of their immunization. There is no follow up for needle stick injury or exposure to contaminated bodily fluids. On one occasion the physician touched the patient chart with soiled gloves, which ultimately contaminated the chart and thus posed a risk to anyone coming into contact with the chart. The care of the patient was dealt with poorly as well. The staff placed and removed IV lines, intubated patients, placed Foley catheter, and put gauze on surgical site- all without gloves. The same syringe with anesthetic was used on multiple patients without sterilization. Distilled water used for irrigation of a urological procedure was exposed to air and then put into an IV bag via a funnel- hair and other particles could be seen in the water. Another major issue observed is that the OR doors are kept open prior, during and post surgery. There is also too much traffic in and out of the OR during surgery with unnecessary people constantly walking in and out and without masks. The OR table was clearly contaminated with bodily fluids and hazardous material and was not properly disinfected while another patient was placed on the same table. The belts and pillows used to harness the patient were soiled and thrown on dirty floor and then reused. Also, the Operating room and the floor are not cleaned (with contaminated sheets and patient fluids on the floor) while another patient is brought into the OR bare foot. Another thing witnessed was eating in the OR. Eating in the OR is strictly prohibited in all health care facilities.
The cleaning and disposal of waste was another area in need of improvement. For example, all waste is combined into one single bag including hazardous, non-hazardous and sharps. There is no sharps container or other labeled waste buckets. The suction bucket is not disposable, meaning that the same bucket is used in between patients without cleaning. At the end of the day, it is washed in the sink with tap water. This exposes patients to blood borne pathogens from patient to patient.
The central sterilization department (CSD) is built in a way that would effectively function for all the hospital needs, however the department setup is not correctly utilized. Figure 1 shows the layout of the department. The sterile storage area is not kept sterile at all because dirty items are directly brought into the sterile area from the OR. The cleaning of items is done in the OR unit, the staff from all areas of the CSD work in all areas regardless of the sterility of the area. The elevator used for transportation of items is used for sterile and dirty tools and linen. The clean changing area is used as a laboratory for tissue biopsies. The sterilization department has the required indicators required for testing tools and machines. First, the cleaning of the surgical tools are put into Glutacide-28 for 15 minutes then put into Descoid and Triacid then washed with water and sent to be sterilized. All this cleaning is done in a room connected to the OR. The disinfectant used is Surfosept with active ingredients isopropanol, propanol, and DDAC. The tools are put into an autoclave at 134 degree Celsius for 3 to 7 minutes and 121 degrees for clothes. After cleaning the indicator used is Hemo-Check S to check for blood residue on items. Three items are randomly chosen from each packet and all three must pass, if it fails the tools are sent back to the OR to be cleaned again. However, the sterilization department had run out of these indicators for 15 days, therefore none of the items had been checked. After cleaning, BAG-Integraph is put on top of the tools then put into autoclave. This will change color from purple to green if the items were properly sterilized and once the items are brought out the CSD employees will know if the tools are sterilized or not. Unfortunately they had no supplies of these left either. The chemical indicator used is BAG-RePAC; these strips are put into each tool batch prior to closing and then put into autoclave. When the packet is opened by the OR staff they will check the strip to see if the color has changed from purple to green-however, none were in stock. The indicators used to inspect the autoclave are BAG-Auto-Check Kit II/7561, a Bowi Dick test at 135 degree Celsius for 3.5 minutes (which lasts about 50 minutes). In 3 to 4 minutes the color should change from blue to black if the autoclave is functioning properly. This is done every morning and recorded. The biological indicator used to test the autoclave is BAG-Bio Check STEAM- if there is bacterial growth in the vial then the machine is contaminated and not functioning properly. This is done once a week on all the machines.
Gulan Hospital in Akre was newer and better equipped than Dohuk. They were able to place sterile sheets on the bed and changed it in between patients. However, the use of gloves and masks was limited in the OR with the same issues as Dohuk. Meaning that IV placemement/removal and medicine given via IV are all done without gloves. There was staff in the OR without face masks on some occasions but not as frequent as Dohuk. However, there were dirty sheets and scrubs left on the OR floor in between patients. The OR unit had separate elevators for dirty equipment and clothes and one for sterilized material sent from the sterilization department. Also, the cleaning of tools was not done in the OR in Akre, it is all sent to the sterilization department.
The Emergency Department in Akre should be completely redone. The physician and nurses do not wear gloves at all. Unqualified non-medical staff, (cleaning staff) removes IV lines and IV placement without gloves. There is no needle-stick injury or exposure to contaminated bodily fluids tracking, record keeping or treatment.
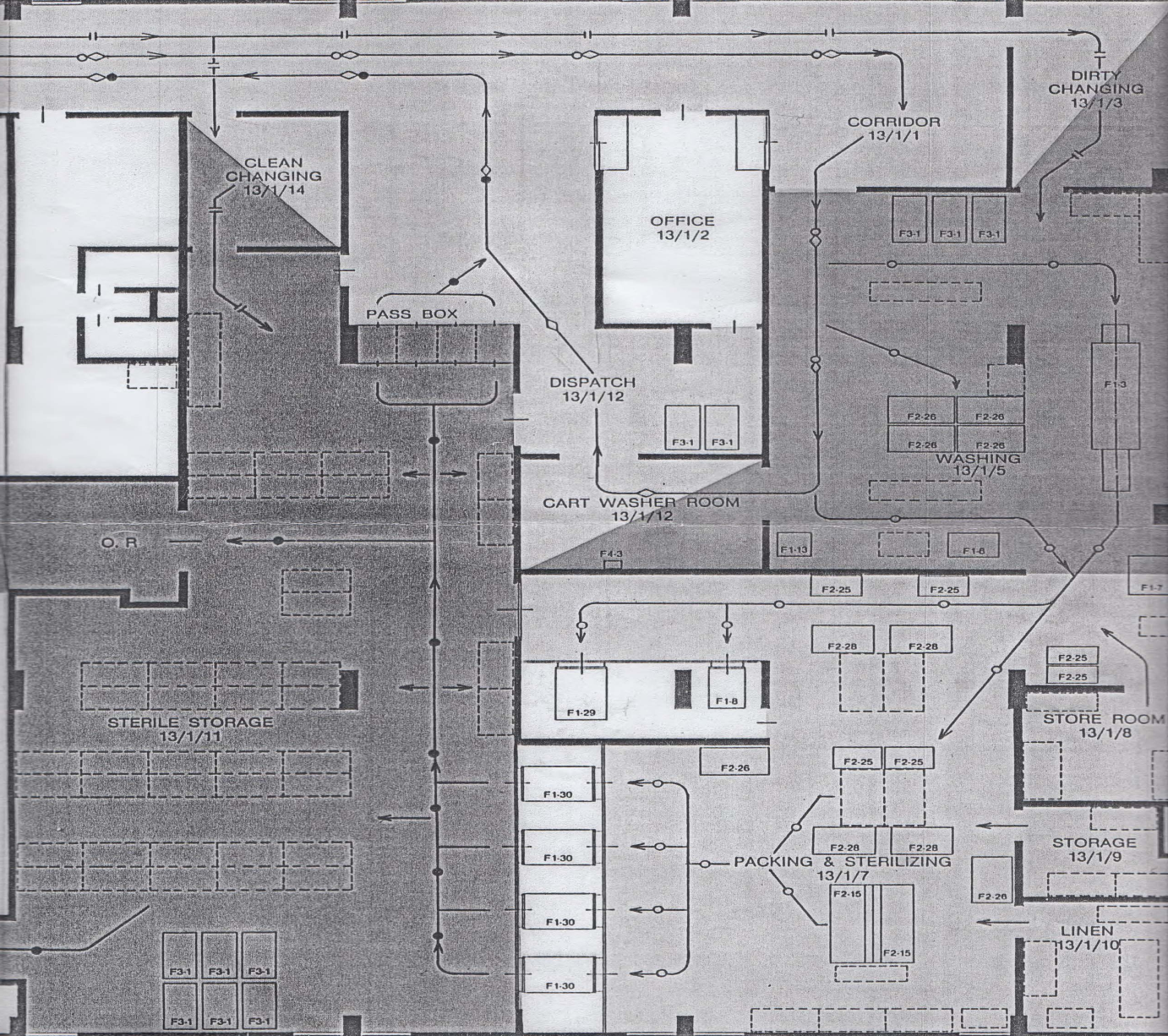
Figure 1: Central Sterilization Department Layout at Azadi Hospital in Dohuk, Kurdistan (Click to enlarge)
Discussion:
The healthcare system in Kurdistan is still in its primitive stages but a careful developmental program needs to begin to provide appropriate care for the Kurdish people. To achieve better Infection control measures the following areas are in need of improvement; education, resources, overload of patients on health care workers, and encouragement from the Regional Health Governor and Ministry of Health.
Sterilization Department:
To begin with the central sterilization department (CSD) is vital for an Effective Control and Prevention program. The expertise and knowledge of CSD personnel is important to ensure high standards of decontamination; because an effective CSD results in long term savings. The goal of a comprehensive infection control program is to minimize the level of contamination in areas that are considered clean activities which would include operating rooms, workings areas for sterilization, storing instruments and other items. Areas in which dirty activities take place include rooms where soiled instruments and other items are washed. It is ideal to follow the layout of the Figure 1 where there are separate rooms-one for receiving and cleaning instruments and other items and other rooms for final sterilization and storage. It should be arranged so that activities and objects flow in an organized way. It is key to have good spatial separation between soiled handling area and the clean, packaging area. Soiled, used and recyclable equipment should be collected from the units and then be transferred to the CSD where it is washed, inspected, disinfected or packaged and sterilized and dispatched back to the units. It is imperative that dirty instruments not be washed on the units- should be delivered to the CSD. Physical barriers should separate dirty and clean areas in the reprocessing room. Air should move from clean area to the dirty are, both areas should have separate storage facilities, patterns developed in which soiled objects never cross paths with clean, sterilized instruments and other items, the doors are kept closed in the reprocessing rooms in order to minimize dust contamination, staff work in either are-never in both (1). Inadequate destruction of pathogens (bacteria, fungi, viruses, spores, and other microorganisms) left on an instrument by one patient can result in serious adverse clinical outcomes in the next patient. The risk is even more acute for instruments used invasively. Single use equipment should be used where appropriate, particularly where decontamination cannot be carried out effectively (suction instruments). Any reusable equipment which is reused and which has been employed for a procedure involving potential contact with a patients (suction instruments and syringes) blood must be sterilized or disinfected before it is reused (7). As with all other contaminated items, clothing and linen stained with blood or other potentially infected body fluids which is to be reused should be handled with care and placed in suitable bags for safe storage and transportation for laundering.
Disinfection/Antiseptics:
Antiseptics and disinfectants are used widely in hospitals and other health care settings for variety of topical and hard-surface applications. In particular, they are an essential part of infection control practices and aid in prevention of nosocomial infections.
Several alcohols are shown to be effective antimicrobials. Alcohols exhibit rapid broad-spectrum antimicrobial activity against non-motile bacteria, viruses and fungi. However, they are not sporicidal and thus why they are not used for sterilization. It is believed that alcohols cause membrane damage and rapid denaturation of proteins with subsequent interference with metabolism and cell lysis (2). Gluteraldehyde, an alcohol widely used as a disinfectant and sterilant for endoscopes and surgical instruments. Iodine, another antiseptic is rapidly bactericidal, fungicidal, tuberculocidal, virucidal, and sporicidal (2). Iodine rapidly penetrates into microorganisms and attacks major proteins. Hydrogen peroxide is a commonly used biocide for disinfection, sterilization and antisepsis. Hydrogen peroxide demonstrates broad-spectrum efficacy against viruses, bacteria, yeasts, and bacterial spores. It attacks essential cell components, including lipids, proteins, and DNA (2).
Precautions:
Universal precautions are an approach to infection control to treat all human blood and body fluids as if they were known to be infectious for HIV, HBV and other blood pathogens. Appropriate action includes the use of gloves, masks and gowns if exposure is anticipated. Standard precautions define all body fluids and substances as infectious. Standard precautions apply to blood, all body fluids, and secretions, excretions, except sweat, regardless of whether or not they contain visible blood, non-intact skin, and mucous membranes (3). Standard precautions are put in place to reduce the risk of transmission of microorganism from both recognized and unrecognized sources of infection in hospitals. Standard precautions include the use of hand washing, personal protective equipment (PPE) such as gloves, masks and gowns. Transmission based precautions such as airborne, droplet, and contact precautions are recommended to provide additional precautions beyond standard ones to interrupt transmission of pathogens in hospitals (3). Transmission based precautions can be used with patients with known or suspected to be infected or colonized with important pathogens that can be transmitted via air, droplets or contact with dry skin or contaminated surfaces.
Health services should have management systems in place for dealing with blood and body substance spills and protocols should be in place and emphasized in ongoing education or training programs. Standard precautions apply including the use of PPE. Spills should be cleared before the area is cleaned to prevent the size of the spill from increasing. In clinical areas (operating rooms) blood and body substance spills should be dealt with as soon as possible (4). Care should be taken to thoroughly clean and dry areas that come into contact with bare skin (such as operating tables). PPE should be used for all cleaning procedures. Hands should be washed and dried after cleaning.
Needle stick/Sharps Injuries:
Needle sticks and other sharps-related injuries which expose workers to bloodborne pathogens continue to be a significant hazard for hospital workers. Data has shown that needle stick injuries occur most frequently in the operating room and patient rooms (5). Employers must maintain a log of injuries from contaminated sharps. Hepatitis B vaccine and vaccination series should made available to all employees with occupational exposure including post-exposure evaluation and follow up- including post-exposure prophylaxis. Some solutions to decrease sharps injuries is to use safer needle devices and proper handling and disposal of needles and other sharps. Sharps containers should be readily available. The sharps containers should be closable, puncture resistant, and leak proof on both sides and bottom. The sharps container should be accessible, maintained upright, not allowed to overfill and color coded or labeled with the biohazard symbol (5). The most important measure whereby health care workers can be protected against Hepatitis B is by immunization, which provides protection in 90% of recipients (7). However, immunization is not a substitute for good infection control practice since it provides no protection against infection with other blood borne viruses. The following measures will help to minimize the risk of exposure to blood borne viruses; washing hands before and after contact with each patient, and before putting on and after removing gloves, change gloves in between patients, cover existing wounds with waterproof dressings, wear gloves where contact with blood is possible, avoid sharps usage where possible, avoid wearing open footwear in situations where blood may be spilt (operating room) or where sharp instruments or needles are handled, clear up spillage of blood promptly and disinfect surfaces, change gloves regularly if performing or assisting with prolonged surgical procedure even if no glove puncture is suspected or recognized.
Surgical Site Infection Prevention:
Surgical site preparation is an important step in preventing infections. Whenever possible, the identification and treatment of all infections prior to elective surgery should be undertaken. Require patients to shower or bathe with an antiseptic agent on at least the night before the operative date (6). Thoroughly wash and clean at and around the incision site to remove gross contamination before performing antiseptic skin preparation. Surgical team members should keep nails short and not wear artificial nails. Perform a preoperative surgical scrub for at least 2 to 5 minutes using an appropriate antiseptic (6), scrubbing hands and forearms up to the elbows. Education and encouragement of surgical personnel who have signs and symptoms of a transmissible infectious illness to report condition promptly to a supervisor. Administer prophylactic antimicrobial agent only when indicated and selection should be done based on its efficacy against the most common pathogens causing surgical site infection. Administer, by intravenous route the initial dose of prophylactic antimicrobial agent so that bactericidal concentration of the drug is established in serum and tissues when the incision is made (6). Maintain therapeutic levels of the agent in serum and tissues throughout the operation and until at most, a few hours after the incision is closed in the operating room (6).
Maintain positive pressure ventilation in the operating room with respect to corridors and adjacent areas. There should be a minimum of 15 air changes per hour, 3 of which should be fresh air (6). Operating room doors should be kept closed except as needed for passage of equipment, direct surgical personnel and patient. Limit the number of personnel entering the operating room to necessary persons only. When visible soiling or contamination with blood or other body fluids of surfaces or equipment occurs during an operation, a disinfectant should be used to clean affected areas before the next operation. Wet vacuuming the operating room floor after the last operation of the day with disinfectant (6) should be done on a daily basis.
Wearing surgical mask that fully covers the mouth and nose when entering the operating room if an operation is about to begin or already under way or if sterile instruments are exposed. Wear the mask throughout the operation. Aseptic techniques should be followed when placing intravascular devices. Postoperatively; there should be sterile dressing for 24 to 48 hours of an incision that has been closed primarily (6). Wash hands before and after dressing changes and any contact with the surgical site. When an incision dressing must be changed sterile technique is required. Finally, educating the patient and family regarding proper incision care, symptoms of surgical site infection, and the need to report such symptoms is essential.
Conclusion:
Demonstration of quality health care includes documentation of outcomes of care. Surveillance is a comprehensive method of measuring outcomes and related processes of care, analyzing the data, and providing information to members of the health care team to assist in improving those outcomes. Surveillance is an essential component of effective clinical programs designed to reduce the frequency of adverse effects such as infection. Conduct on-going risk assessment, identify, and implement interventions and strategies to reduce infection risks. Using information gained from the surveillance and a model for continuous improvement, hospital administrators can continue to refine and improve upon the infection record in the hospital.
It is strongly recommended that every hospital should have an Infection Control Team which has the primary responsibility for and reports to the chief in charge, all aspects of surveillance, prevention and control of infection in a hospital. The Infection control team should advise managers and employees on suitable immunization policy. The chief in charge must ensure that all parts of the organization have suitable health and safety policy and that its implementation is monitored regularly to ensure its effectiveness.
*This paper was prepared under the supervision of: Dr. Abdulrahman Tawfeeq Saadi, Assistant Professor in Medical Microbiology & Infectious Control/Faculty of Medical Sciences at Dohuk University in July 2012
Dezheen Zebari is a 4th year medical student at New York College of Medicine. During her second year of medical school she went to Kurdistan to research this paper.
References:
(1) Cleaning, Disinfection, and Sterilization of Medical Equipment. Dec. 2009. Egyptian Medical Syndicate. June 25, 2012. www.ems.org.eg/esic_home/data/giued_part1/Cleaning.pdf
(2) Antiseptics and Disinfectants: Activity, Action and Resistance. Jan. 1999. Clinical Microbiology Review: American Society of Microbiology. June 25, 2012.
(3) Healthcare Wide Hazards: Universal Precautions. US Department of Labor: Occupational Safety & Health Administration. June 25, 2012.
(4) Appendix 5: Procedure for managing spills of blood and body fluids/substances. Feb. 10, 2007. Infectious Diseases: Epidemiology and Surveillance. June 25, 2012.
(5) Healthcare Wide Hazards: Needle Stick/Sharps Injuries. US Department of Labor: Occupational Safety & Health Administration. June 25, 2012.
(6) CDC Recommendations for Prevention of Surgical Site Infection. Mangram AJ, Hospital Infection Control Practices Advisory Committee (HICPAC) and Centers for Disease Control and Prevention (CDC). 1999. Guidelines for Prevention of Surgical Site Infection. June 25, 2012.
(7) Protection Against Infections with Blood-borne Viruses. UK Health Department. Guidance for Clinical Health Care Workers: Recommendations of the Expert Advisory Group on AIDS and the Advisory Group on Hepatitis. June 25, 2012.
